
Prognosis was unfavorable in the pre-antibiotic era. After the introduction of beta lactamase resistant antibiotics, the mortality has significantly reduced, albeit, with appropriate antibiotics and therapy, mortality has been reported to be between 5% and 18% [2]. If left undiagnosed or untreated, LS is fatal.
Conclusion
Most cases of pharyngitis in the pediatric population are viral in etiology and are usually self-limiting without any complications. Presence of atypical symptoms/prolonged or worsening symptoms, warrant a detailed evaluation to exclude the possibilities of coexisting bacterial infections, of which LS is one of the grave forms. It leads to systemic thrombophlebitis and thromboembolism and can be fatal. Therefore, a high index of suspicion is required to ensure timely recognition and appropriate management.
Funding Source: No funding was secured for this case report.
Financial Disclosure: The authors have no financial relationships relevant to this article to disclose.
Conflict of Interest: none
Clinical Trial Registration: Not applicable.
References
1.Tiwari A. Lemierre’s Syndrome in the 21st Century: A Literature Review. Cureus. 2023 Aug 18;15(8):e43685.
2.Allen BW, Anjum F, Bentley TP. Lemierre Syndrome. 2023 Jul 31. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan.
3.Foo EC, Tanti M, Cliffe H, Randall M. Lemierre’s syndrome. Pract Neurol. 2021 Oct;21(5):442-444.
4.Kliegman, R. M., & St. Geme, J. W. (Eds.). (2024). Nelson Textbook of Pediatrics (22nd ed.). Elsevier.
5.Johannesen KM, Bodtger U. Lemierre’s syndrome: current perspectives on diagnosis and management. Infect Drug Resist. 2016 Sep 14;9:221-227.
Figures
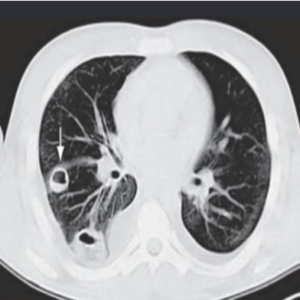
Fig 1: CT chest demonstrating nodular pulmonary infiltrates, suggesting metastatic pulmonary abscess in patient with LS.
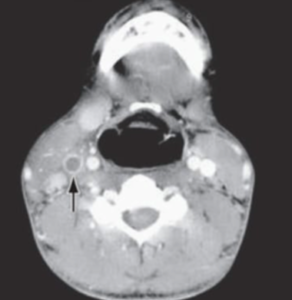
Fig 2: CT neck demonstrating the right IJV thrombus